


Digital Health Business - Dr. John Danaher, President at Adtalem Global Education, former President of Global Clinical Solutions at Elsevier
The Education & Training market

New episode in ‘Digital Health Business’ series by Arkin Digital Health.
(“Miniseries of interviews with industry leaders, coming from different parts of the US healthcare ecosystem, hopefully to provide Israeli entrepreneurs, investors and the Israeli healthcare community insights on the business side of digital health.”)
In this episode we have Dr. John Danaher with us. Dr. Danaher is the president of Adtalem, one of the largest educators of doctors and nurses in the US. He has a exceptional experience in the medical education field with senior leadership positions in industry leaders such as Elsevier, Kaplan and WebMD. He also held numerous board positions in for profit and non-for-profit organizations and even held a fellowship position in the white house.
We tried to understand from John how the medical education and training market responds to the shortage in labor and physicians’ burnout, what are the opportunities in this market and had a particular focus on decision support tools, per the prevalence of (Israeli) companies that are trying to offer such solutions.
You can listen to the interview(s) and follow the series via -
Also, if you are not already subscribed to this blog, you can use this link to easily receive new posts!'
Nadav: we are hearing more and more about labor shortages these days. And obviously, they affect providers in so many ways. How do you see the education and/or the training aspects of this problem?
John: The shortages of caregivers was accentuated and brought out and exacerbated by COVID. Let's focus on US. There's about 100,000 physicians missing today. There's huge shortages in nursing, maybe even 200,000 plus by 2025. The reasons for it are a couple of fold. We're at 330 million Americans. More of that population is, is becoming elderly. And as we both know, the elderly have a number of complex conditions. It's not one. So if you're a physician or a nurse, you're finding yourself increasingly stretched, you're increasingly finding out you've got more work with less resources, etc. On top of it, the best nursing schools or the best medical schools in the US don't have a mission to be a workforce solution. Success is often “generating” a faculty member doing research, etc.. So there's a tremendous opportunity to be a true workforce solution. One last thing that I would say is that when you when you look in the US, it's less that there's a shortage of doctors and nurses in the very affluent areas where they tend to be shortages are in the communities that are lower socioeconomic. So the last thing I would say is clearly what we're seeking to do whenever we can to apply technology in the forms of content management systems, learning management systems, adaptive learning solutions, etc., to constantly be using and leveraging technology in the education of our students.
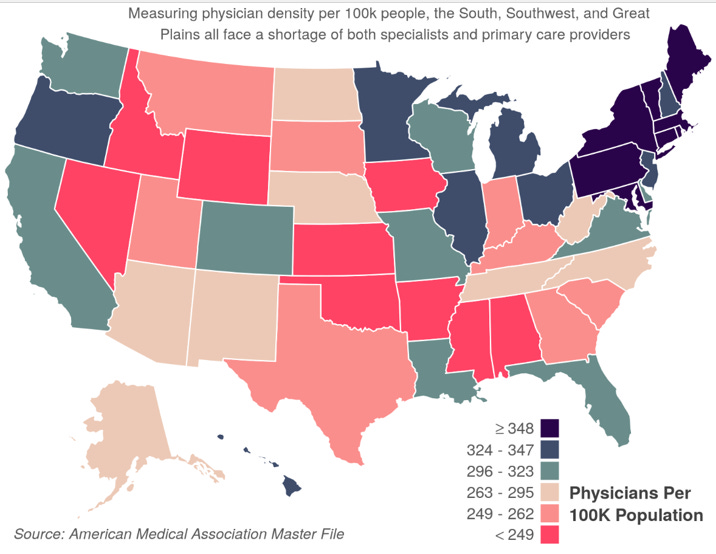
Eve of COVID (EOY 2019) numbers just to give some taste
Nadav: So where do you see opportunities for tech first companies? Do you see them trying to shorten medical training duration? Do you see them pushing healthcare professionals to practice on top of their license? Do you see them perhaps tackling operational related burnout?
John: I think it's all throughout. To be able to get real world data, real world analytics on learners to provide efficient learning experience, you must have a platform that is serving up content in a structured way and then collecting that data, seeing where students are struggling and making sure faculty and administrators have access to that data so they can intercede in real time.
The second area that I would talk about is clearly the area of simulation which is just blown up with exciting, new, immersive experiences that students and faculty have.
To really train and educate physicians we must have enough hours of real world practice. Thing is getting clinical spots is a tremendous challenge and simultaneously many states are starting accept the fact that you can do that on simulators. You remember this when you were training as a physician, when you are doing your rotations as a medical student, for example, you don't always see the range of cases you're going to face when you actually start practicing or even tested. That's the beauty of simulation that you can really serve up exactly and call out the learning lessons. It's really all about giving people a real life experience and then collecting the data and running analytics to see where they're succeeding and where they're where they're struggling.

The important thing, I think, is convincing people with real data that students who use these simulations go on to pass the USMLE or other “high stake exams” at the same rate or higher than students who don't.
Nadav: Perhaps another question which relates to couple of these points you just mentioned, analytics and showing the outcomes and so on. I think that throughout your time in Elsevier, you've touched the area of decision support systems quite a bit and Elsevier is doing a lot of things in this space. What can you share these tools? In Israel, there are many companies in this area from different reasons. So we see a lot of challenges around, market penetration and customers being not so receptive, not so willing to pay and so on. I'm very curious to learn from your experience

Some color why DSS is complex
John: I am actually a huge supporter and believer in clinical decision support and it's really for two reasons. The problem we're trying to solve with CDSs is unintended variability in the delivery of care. I'll say this kind of jokingly, if there is a patient with metastatic breast cancer, there's 25 oncologists, there will be 27 different opinions on how best to do that. One of the benefits of CDSs is that they're providing current evidence based medicine. And, you know, it's not it's not that difficult, perhaps in areas of treating pneumonia or another common condition. But in terms of the cancer therapies that are changing very, very rapidly for example, even the foremost oncologists benefit from having CDSs.
The second thing about CDSs, which is really exciting, is there's a number of regulations in the US, one is them is PAMA, for example where the government actually requires to use decision support tools. And the idea there is to reduce all unintended or all the unnecessary X-rays and imaging studies, etc., and just make sure that what they're reimbursing for with Medicare is justified (clinically). Meaning there are financial reasons in the US to adopt CDSs and to utilize CDSs.
Now there's lots of reasons for resistance, but I think that really the movement is towards CDSs.
(I’ve touched the area of CDSs more extensively on another post)
Nadav: Let’s speak about this resistance, in particular with respect to Israeli companies. I'm sure you've encountered through your time developing and selling CDSs, some challenges and obstacles. I would love to hear your take on that.
John: Nadav, I have been blessed to not only work with companies in the Arkin portfolio, and to work with other Israeli startups. I even had the pleasure of meeting you at Clalit prior to COVID. The innovation and the creativity in Israeli HIT space is second to none. It's the best. And part of it is having access to data sets and the fact that the data sets have been digitized for, I forget whether it's the last 30 or 40 years. However, there are couple of significant challenges for Israeli companies.
The first is to capture a major market.
Now, it's wonderful to have a reference account at Intermountain or at Mayo clinic. But those often take a tremendous amount of work to get up, to get going, etc., and they have huge reputational effects. But really the challenge is, is how do you scale? And sometimes the amount of energy and resources and funding that goes into pleasing one of those 800-pounds entities is not where you want to go. It’s a great reference account but what you quickly realize is selling into those marketplaces may have long sales cycles. It's often more the medium sized hospitals or the medium sized health systems that don't have marquee names, that are quicker to scale and quicker to get up to speed. These accounts come with pluses and minuses of course.
The second thing I think really important is moving to (being based in) those markets. Having a senior executive in the US is very hard, it's very hard to manage and grow. The first (US) hire early stage companies usually pursue is around sales. And that is a flip of the coin because finding really good salespeople is hard in general. Even more so when done remotely. When you're based in Tel Aviv, say, and you're hiring somebody in NY to begin scaling and building up your sales force, it's a crapshoot. I think you reduce the chances of failure if a senior executive from the company is established in the US from an early stage and can meet people and build out the salesforce and the rest of the team.
Nadav: with respect to being in the US I can only share that we're share very similar mindset per my recent relocation to NY.
Final question – What are the areas you think entrepreneurs should avoid?
John: I think there is one area that is not so much ‘not to be in’ , but one have to consider a transition in strategy if in it and that's digital health media for pharma.
There's only so many blockbuster drug launches a year and those are the main drivers that for digital media. What I've been very surprised about is the people who are in those traditional digital media companies are just in the early stages of appreciating and understanding the data that they're sitting on. Pharma companies are becoming more and more conscious of the value of this real-world data. What I'm wary of paid media companies is they often don't have the expertise, the knowledge to really unlock and take advantage of the data they (can) generate.
That’s it for a conversation that started with medical education and training continue to the clinical decision support system and ended with pharma sales and marketing.
Next episode will feature Dr. Amy Abernethy, President of Clinical Studies Platforms at Verily Life Sciences and former Principal Deputy Commissioner & Acting CIO of the FDA.
Stay tuned!
If you are enjoying this blog, it would be really helpful if you can share it with relevant people.
As always, would love to hear your thoughts and feedback!
Thanks,
Nadav
EMR is the most underutilized tool in medical education. it really ought to function as the modern interactive textbook if designed properly.
Ch 10 in Innovator's Prescription mentions how health systems will begin training their own workforce because incumbent institutions cannot keep up. Oak Street Health already has NP program https://www.oakstreethealth.com/nurse-practitioner-training-program. Christensen makes a convincing argument about having variable training with certain results (eg Toyota) over fixed training with uncertain result (which is the current edu system we have).