


Vaccines, value-based care… and Israel
Why COVID vaccination rate in Israel is 740% higher than in the US and how it is related to less discussed merits Israel has that can leapfrog value based driven global ventures?

Late night, the kids are asleep (finally!) and it’s yet another COVID lockdown in Israel. Seems like the perfect setting for a new post...
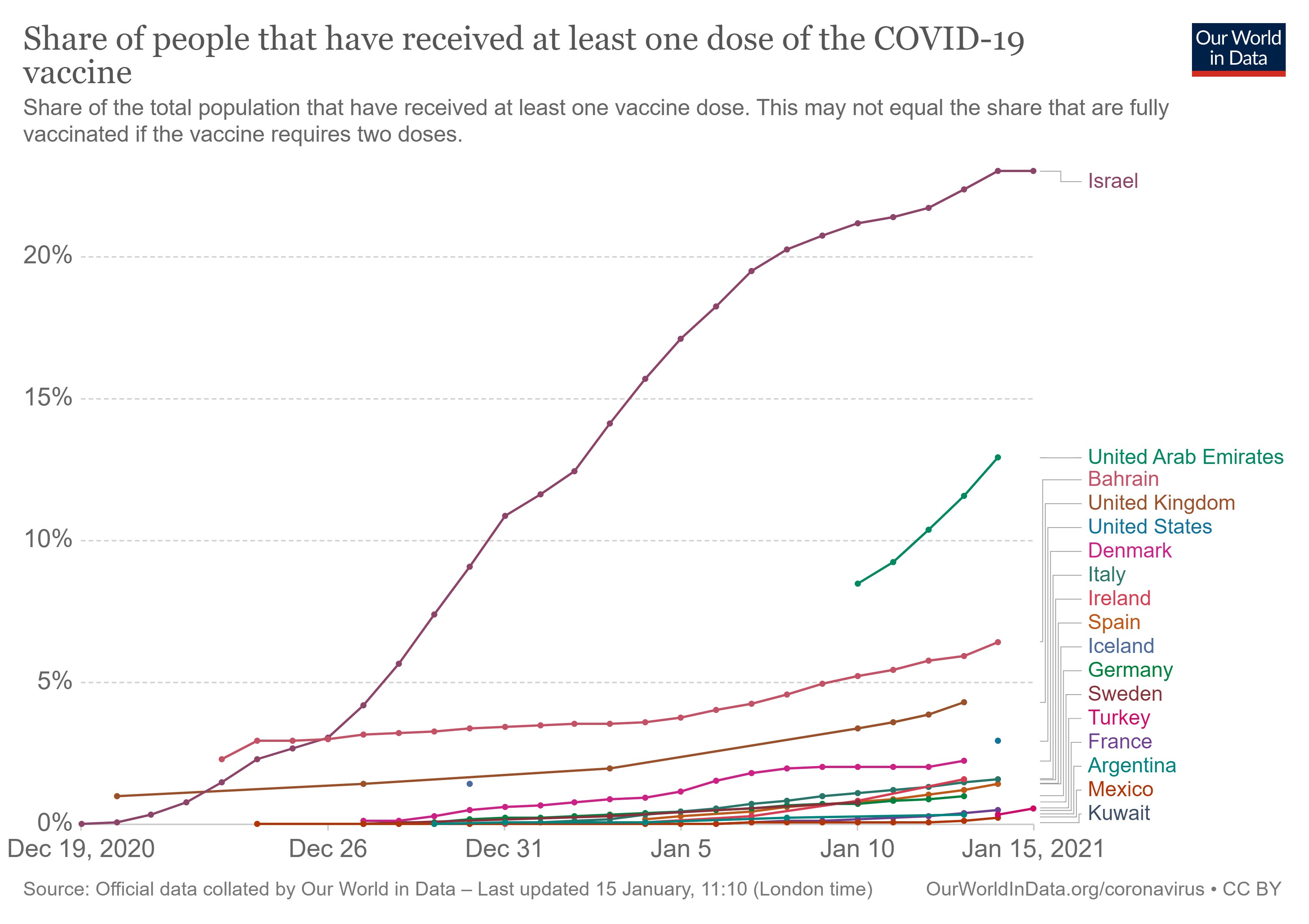
The last two-three weeks have been all about the vaccination operation in Israel. Much has already been written about the truly “warp speed” pace (23% of the population already vaccinated, with a non-comparable ramp up pace as illustrated in the figures below). Even when discounting to its small geo-demographic size, the statistics are still remarkable.

The purpose of this post is not to praise this achievement (although it is nice to have some good news these days) but to extrapolate why it may be good example for the perhaps less spoken merits Israel possess as a digital health launch pad.
To do so, it is first important to understand the foundations of the Israeli health system, and to single out some special features that essentially created the perfect setting for such operation. In other words, let me try to convince you why this outcome is not surprising at all.
Community and primary care as THE cornerstone
The Israeli health system is based on the “national health insurance law”, acted on January 1, 1995. In its very first line it is emphasizing the system’s core values – “Justice, equality and solidarity”. These values are derived from the history of our health system, which has been running even before the establishment of Israel as a country. The law stipulates that the state is responsible for insuring health of all its citizens and permanent residents by a universal coverage of "medical services package“ (e.g. treatments, services and medications). This “package” is provided by 4 sick funds (akin to HMOs) which are funded by the government through a capitation formula that only considers limited socio-demographic parameters.
Now, why is that important?
In essence, two integrated payer-provider organizations (Clalit, Maccabi) are responsible to provide health service to 75% (!) of Israelis. That’s like Kaiser Permanente and Intermountain Healthcare (both being IDNs, kind of like the formers) providing care for 250M lives (and not <15M). Even the entire Medicare population is <20% of the US population and there are countless organizations that support it. But wait, that is not even the interesting point. Because the sick funds are paid by the government throughout a capitated model (~$1500 per member), excluding ANY complex illness or excessive healthcare utilization, they have (almost) ZERO incentive to offer unnecessary services. In other words, the very opposite of fee-for-service models.
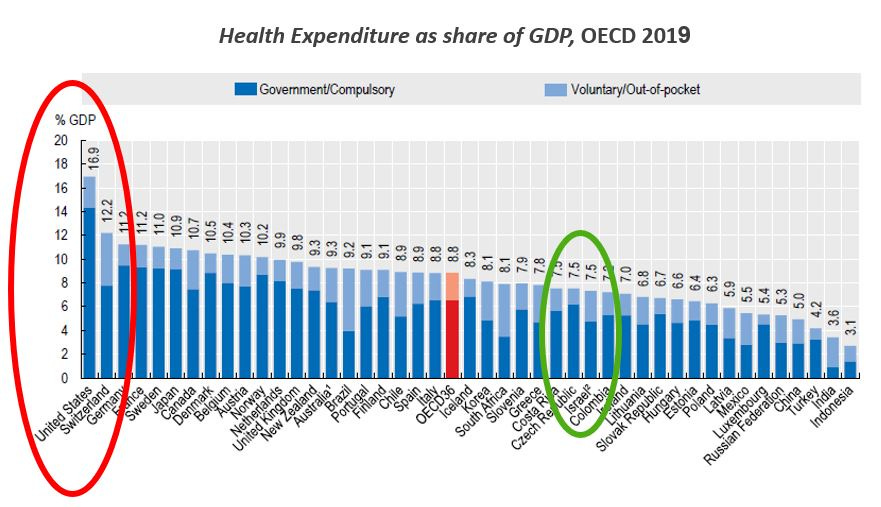
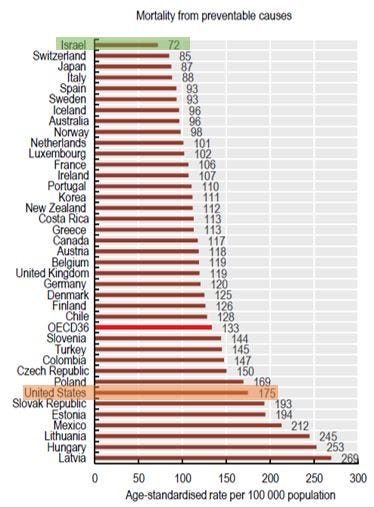
As a derivative, the Israeli health system is operating on a narrow budget, yet there is no compromising on quality. Israel is constantly ranked high in several health outcomes indices such as life expectancy, infant mortality, rates of age-adjusted mortality from CV diseases and malignancy, and more.
Furthermore, attrition rate between sick funds is ~1% annually and thus membership is usually life-long (vs. ~2-3 years in the US) and cross families. The result is a structural financial incentive to keep people healthy and outside the hospitals and thus alignment of interest on preventive (proactive) primary care.

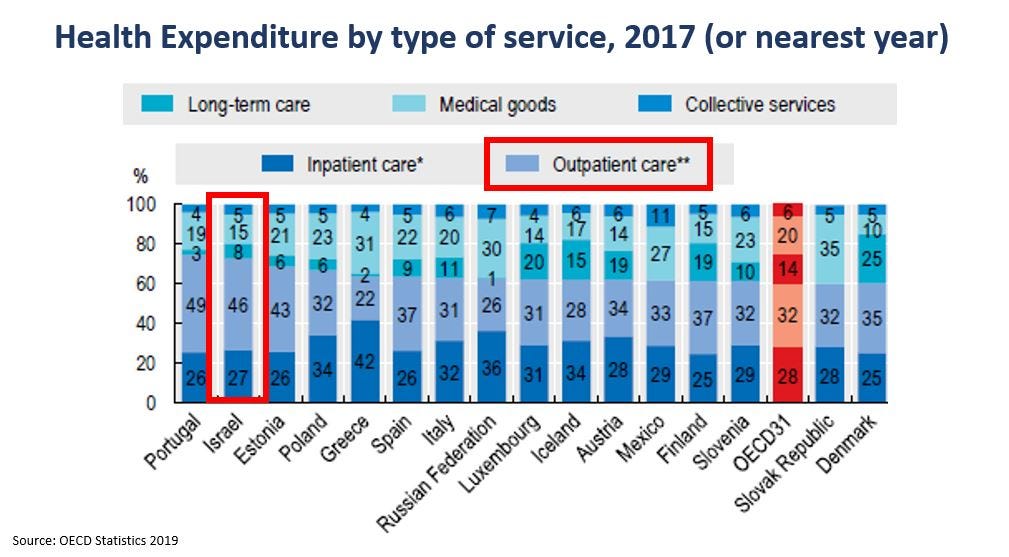
To provide such care, the sick funds and the country have been heavily investing in community care in a disproportional manner to other countries. Currently 90% of community services are administrated by public entities (that is, non-private and really non-for-profit). The importance of primary care is embedded within the training of medical staff in Israel, stressed as the “front line” that will determine the quality of the entire system. Perhaps the most distinctive notion is that family physicians (all PCPs in Israel are “family doctors”, no such entity as “general practitioner”) earn on average more than surgeons!
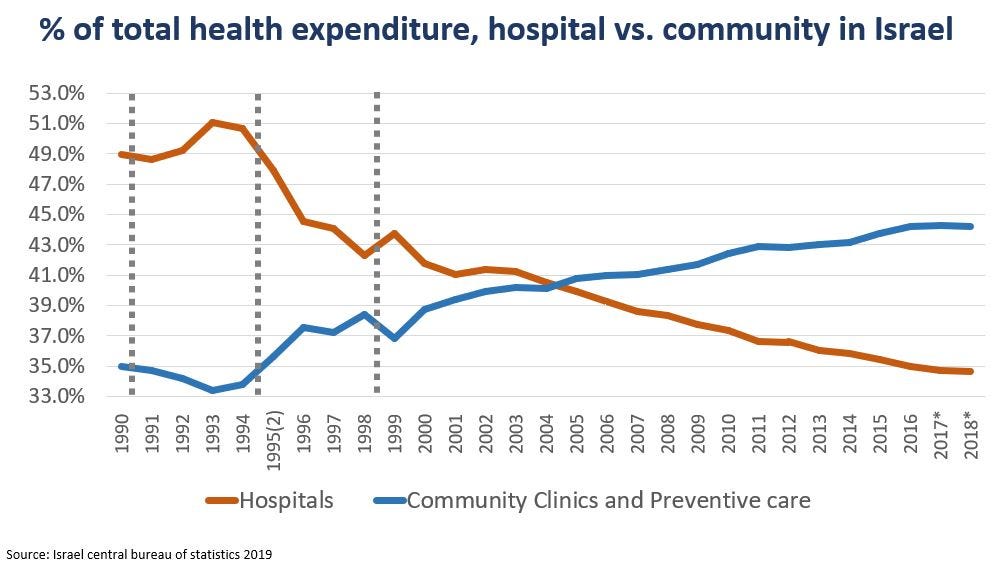
The inherent need to provide the best primary care is also a core driver for the digitization of the Israeli healthcare system more than two and half decades ago. A robust digital infrastructure is critical for supporting patients throughout their entire care journey. Clalit, with its 4.5M members, has had the same two EHR systems for more than 20 years: one for in-hospital and one for community care. And they are connected.
Taking all that in mind, more than 100K vaccinations per day from almost day 1 seems not like a coincidence rather than an expected by product. You have the physical infrastructure (community care), you have the data to support it and on top of all, you have alignment of incentives. Bingo.
Value-based care sand box
Let’s pause for a moment and talk about value-based care.
VBC is far from being as predominant as projected few years ago. Although COVID has created some tailwinds (as fee-for-service businesses suffered a major hit due to the reduction of ambulatory procedures for example, and also) it seems safe to state that (1) VBC is very underutilized, (2) it is not a big surprise per the misaligned incentives between payers-providers-patients in the US and (3) it is a growing market. Consequently, there is a gamut of new entrants, supported by loads of $$$, trying to tap in or to create value-based opportunities - digital ACOs (Aledade), care-insurance navigation (Grand rounds, Eden, Alignment health), digital IDNs (Bright Health, Devoted) just to name a few.
Part of the reason they are so capital intensive (these six companies alone raised more than $3 BILLION!) is the challenging exploration phase and the need to lay many foundations to crystallize their value proposition.
Now, wouldn’t it be just great if there was a crystal ball to help understand how value-based advantages and disadvantages would look like, and thus reducing initial burn rate / time to product market fit / unfruitful endeavors? I would argue that this is the kind of potential Israel possess.
Let’s reconsider the foundation that allowed the rapid vaccination in Israel as presented above: coordinated and preventive focused system, working in a digitized manner for a long period of time. In essence, a value driven system with the infrastructure to allow it.
(bearing in mind that there is almost no fee-for-service and payers/providers are incentivized by their capitated budget to keep people healthy, as in VBC)
Consequently, Israel has untainted longitudinal data for in-silico ideation (very low attrition rate, no incentives for up-coding per capitated budget), and the physical infrastructure for real world POC. This is like having counterfactual reality of value-based system in a highly venture friendly (“start-up nation” …) environment. Think of “back to the future” without using the Delorean.
Potential and real life
By all means, I don’t suggest that Israel is a “general VBC emulator” for the US or any other health system. That would be oversimplification of a VERY complex situation. But I do think that for certain well-defined use cases Israel can serve as a great “shortcut” to jumpstart and establish the validity of value-based centered ventures, as long as few factors are addressed:
As a starter, the process must be executed with a preliminary and then complementary endeavor in the target market for customer discovery and validation (because Israel by itself is too small in most cases to serve as the market). The insights generated from both ends must be converged correctly into a single canvas. In particular, one needs to understand the specific use case (i.e., the problem), IF and how it can be emulated or better understood via the combination of data, system structure and accumulated knowledge of best practices.
To emphasize, this is not a “give me as much data as possible” concept. This notion has long been dissolved. So yes, the Israeli health system has an abundance of available data but most of it will not be relevant for multiple reasons (different population characteristics, physicians’ tendency or obligations, data architecture, different language just to name a few). There must be a clear understanding why and how (using propensity scores and different calibration mechanisms for example) a specific data set would be useful as a possible counterfactor reflection of the target market. Sadly, many startups fail in this process and waist precious time and resources on futile pilots.
Finally, you need to understand what service / system feature could in fact be relevant in the foreseeable future. In other words, what common practices in the Israeli system that will be incorporated in the target market in the next 5-10 years. While doing that you need to consider the difference in demography vs. geography (9 million people on a small piece of land) culture and accumulated experience of providers / administrators per the inherent learning curve in many cases.
This might sound like a big blurb so perhaps an example would be useful.
Tyto care was born about a decade ago when telemedicine was already an existing reality in the Israeli system but really scarce in most US and EU. Again, because the importance of community care and the need to keep people out of the hospitals, there was a clear incentive to establish this modality so early.
Tyto founders hypothesized (remember that was a decade ago…) that prevalent telemedicine utilization will not stay a distinct feature of the Israeli system but in the (near) future will expend in larger markets. With this notion in mind, they had an exceptional opportunity to improve their offering based on real world experience, as they could:
Understand what are the consequences of telemedicine visits, what are their advantages but also their downsides, and how do they differ between children and adults.
Extrapolate that in the foreseeable future (today) there would be a great value to augment the e-visit with the capability to do even part of the physical exam.
Create a nationwide pilot with Clalit (>50% of the Israeli population) about 4 years ago and improve the product based on real world evidence (that would in fact reflect the future situation in other markets).
Infer and proof the value of adding their solution to that workflow. In particular, how incorporating remote throat, ears and lung inspection to e-visits could drive down unnecessary healthcare utilization (E.D. visits, hospitalizations, etc.)
Be best-positioned to bank on the (post)-COVID surplus of telemedicine.
(Tyto has successfully launched in the US and Europe and the company raised $105M to date).
Closing remark
This post covers an idea I’ve been playing with for a time now. I’d very much appreciate any feedback for better or worse. It is always highly beneficial to have a sanity check. Thanks in advance.
Twitter: @Nadav_Shimoni_
LinkedIn: https://www.linkedin.com/in/nadav-shimoni-m-d-03992489/
Want to have these posts directly to your mailbox?